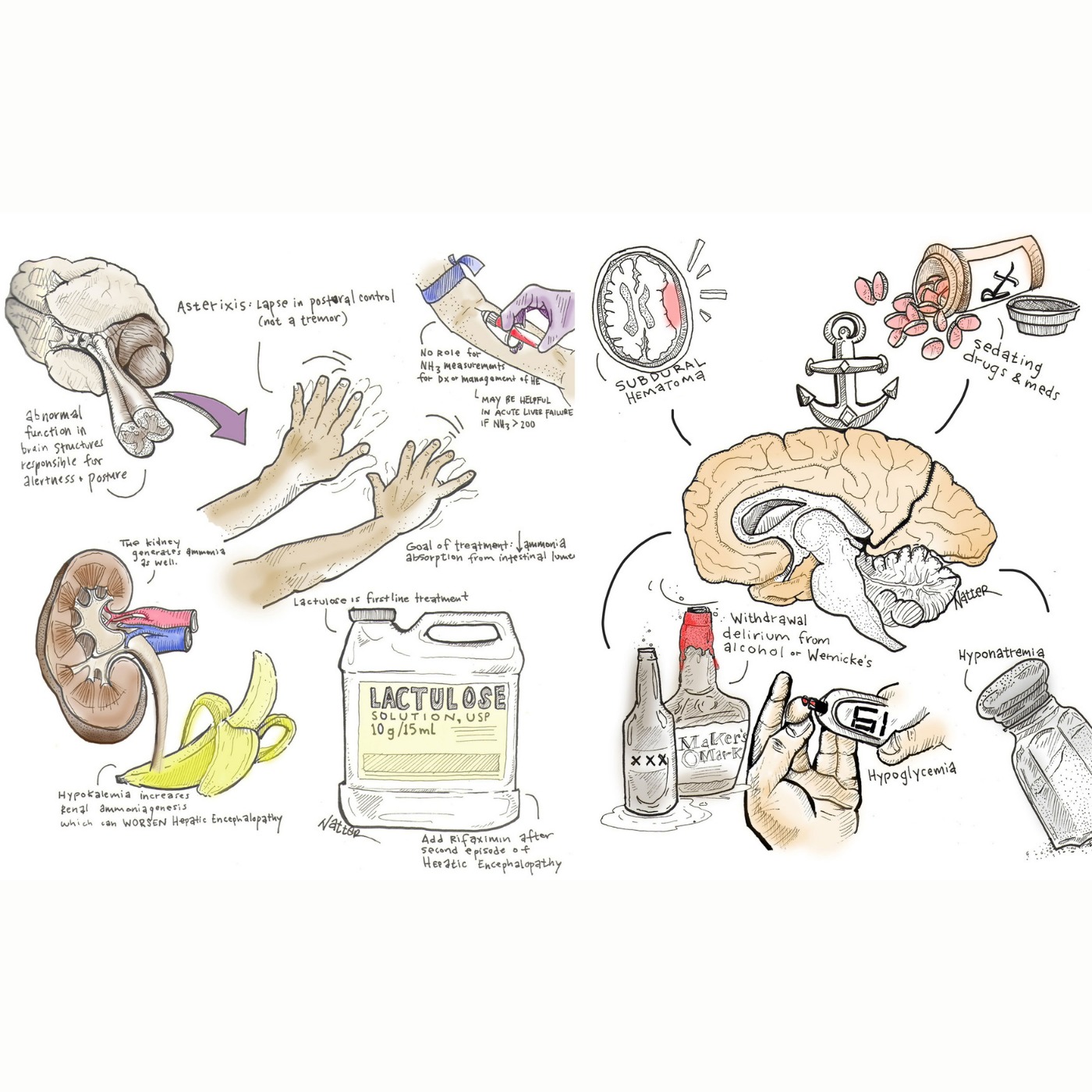
Hepatic encephalopathy (HE) diagnosis and management are explored, emphasizing the importance of considering alternative diagnoses for altered mental status in cirrhotic patients, such as brain bleeds, Wernicke's encephalopathy, or sepsis. Asterixis, a sign of HE, is clarified as a lapse in postural control linked to brain structure dysfunction, while also acknowledging that it isn't exclusive to HE. Treatment focuses on reducing ammonia absorption using lactulose as a first-line treatment and rifaximin as an add-on after the second HE episode. The discussion highlights hypokalemia's role in stimulating renal ammonia production, stressing the need for potassium level correction. Serum ammonia levels are deemed to have poor discriminatory power in HE, except in acute liver failure cases, where elevated levels indicate a higher risk of cerebral edema.
Sign in to continue reading, translating and more.
Continue